Dr.Mike Yeadon' s Key Testimony - Part I - III
Source: https://www.ukcolumn.org/article/dr-mike-yeadons-key-testimony-part-i-the-eight-covid-lies, https://www.ukcolumn.org/article/dr-mike-yeadons-key-testimony-part-ii-vaccine-damage, https://www.ukcolumn.org/article/dr-mike-yeadons-key-testimony-part-iii-the-hot-lots
Part I: The Eight Covid Lies
Published: January 11, 2022
This is the first instalment of a five-webpage transcript of Dr Mike Yeadon's testimony to the 86th session of Stiftung Corona Ausschuss, held on 7 January 2022.
In this transcript, covering the first twenty minutes of his testimony, Dr Yeadon establishes his credentials and rebuts critics of his motives.
Career
I'm Dr Mike Yeadon. I describe myself as an industry veteran. I worked in the biopharmaceutical industry for all of my life.
My first degree was biochemistry and toxicology. English people don't like to brag, but I’m told I should. I was top of the year by a very long way.
As an undergraduate, I worked under military clearance at Porton Down: that's the equivalent of Fort Detrick. It’s where the UK military develops its so-called chemical defences. So I was under the Official Secrets Act—they must have thought I wasn't a crazy person at the time.
I also worked for six months at the Police Forensic Service headquarters at Aldermaston, so i learned a lot of analytical techniques in that time.
Then I did a research-based PhD in respiratory pharmacology, and after that I jumped into industry. I had seven years, seven happy years, at the Wellcome Research Labs, before they closed after being acquired by Glaxo. So my my career spanned the consolidation phase of pharmaceutical companies—we call it the “dirty snowball”. Companies became absolutely huge, and that's relevant to what's happening today: they are so large, so powerful.
After that, I went to Pfizer in the UK, at their very famous Sandwich, Kent, research base. I think more blockbuster drugs were discovered and released from that lab than any other single establishment on the planet. I wish I could claim I had anything to do with it, but I didn’t. But what [that job] did do is give me the opportunity to learn, as it were, at the knee of great drug discoveries. People [at that laboratory] actually conceived and led programmes, invented molecules, developed them, went through safety testing and launched them. And they all made more than a billion a year thereafter. So it was a really good place for learning this trade.
I left Pfizer in 2011, having been head of respiratory research worldwide. So I was the chief scientific officer for that therapy area, Allergy and Respiratory. I left because they closed the site in 2011. I played an important role, I think, in helping some of those programmes, and some staff, to move to new homes: the world's second largest generics company, Mylan, acquired some space on that research park and hired many of my former colleagues. Obviously, I didn't do the deal, but I had, I think, something to do with [the success of] pitching it to the company.
Over the next ten years to today, I’ve been a consultant to startup and mid-phase biotech companies. Some are now public, others privately held. That's about thirty companies, mostly in the field of respiratory or inflammation, immunology, that kind of thing. In the middle of that ten-year period, I had the opportunity to start my own biotech company with three other colleagues, and to raise some money from private venture capital and so acquire some compounds from my former portfolio, because Pfizer was closing the site down and indeed shrinking its footprint. That was quite a common model ten years ago.
So that's me: I have the broad biological discipline and understanding necessary for doing research—that's understanding disease and mechanisms well enough to contemplate intervention points that could help slow down a disease or ameliorate symptoms. And to do so safely: that was always the number one watchword.
Refutation
Some people have said, “Why are you speaking out?” and, “You're a crazy person!”, or whatever. The three things, I would say, most commonly attributed to me which are not true, I will take them [in turn]:
- “He's a bitter ex-employee.” — Well, you know, for one, I left ten years ago. I don't hold a grudge, and certainly not for ten years. Secondly, Pfizer and I got on really well. I would say—to this day—that Pfizer was the best employer I ever worked for. It's a fantastic place to work. For the reasons I described, something's gone wrong since, obviously; but I was unhappy that I had to leave. They were very good to me.
I was one of the last employees off the site, because I was helping place people and projects. So that doesn't sound like a bitter person. They also treated me very well in terms of redundancy, because I was a vice-president.
And then, as I’ve said, a year after leaving, I came back with money and a lawyer and did a deal with them, and then two years later they put additional capital in. That doesn't sound like we're getting on badly. And in 2017, when Novartis acquired Ziarco, my biotech, they made an undisclosed sum that I would say would make them very happy. They definitely did a good deal. That was five years ago, and I’ve had no interaction with them since. So no, I’m not bitter, and I was very lucky to make some money: that's what has allowed me to be independent, by the way.
- Others have said I’m “seeking fame”. — Well, no. Despite the fact that I can appear on TV or on camera, I’m actually by nature quite a shy person. If you left me to my own devices, I’d be tinkering with motorbikes in a shed, probably. That's what I like to do.
- And others say, “Well, he's making money.” — No. There's not a single thing I’ve ever done [in media appearances] that has been monetised, and indeed I probably lost hundreds of thousands of pounds being thrown off the scientific advisory boards of former clients [since speaking up about gene therapy injections], when they said, “You've become the story and it's not acceptable,” which I understood.
So it's costing me money; it's hurting my reputation; and I had every reason just to stay at home and enjoy my early retirement. No, the reason I’m speaking out is because I noticed advisors to the UK Government lying: lying directly on television.
At first, it was just kind of fascinating, but through the spring and into the summer of 2020, I became first alarmed and then later in the year frightened—and I still remain frightened.
Co-ordination
Why? Every [developed] country had [before Covid] what was called a pandemic preparedness plan for things like this, or influenza more typically, and I’ve read them. I’ve read all of them, maybe twenty, from the G20 countries, plus the WHO [pandemic preparedness plan]. And in essence, they have only two things to recommend:
- If you are symptomatic, please stay home and away from other people until you're better—and that's because we've known for decades that symptomatic people drive respiratory viral infections, epidemics.
- Wash your hands more frequently than usual—because with any new pathogen, we don't understand transmission properly, so that's a good precaution.
The next nine pages of these [pre-Covid] pandemic preparedness plans involved telling us what [countries] shouldn't do. None of them involved: border closures, unless you lived on a small island; school closures; business closures; mass testing of the well; lockdown; masking; anything like that. None of them. Absolutely all of the things that we have been told are “essential” were missing and explicitly ruled out by the previous plans.
So I would say the strongest evidence I can offer for my assertion that there is a supranational plan to take over all of the liberal democracies is this that all of the countries had somewhat similar pandemic preparedness plans, that were very simple, and they all discarded them in the [same] weeks of March 2020. All of them. And they replaced them with the same narrative script.
Lies
I’ll just describe [that script]: what I call them the the Eight Covid Lies. Every single one of them is an untruth. And I think the objective was to frighten people to death, and I think it's worked.
So how could it possibly be that Germany, Italy, the United States, Iceland, Scandinavian countries, have all got the same bunch of wrong information, all at the same time? I put it to you, ladies and gentlemen of the audience, that there's only one way that can happen: and that's if they all agreed to do it beforehand, really.
I’m not going to take a lot of time on the Eight Covid Lies today, because there was a very long recording on The Highwire with Del Bigtree, about a year ago, where I go through them in painful detail. But, [in summary,] what did they say?
1. Well, they told us things like: “This is an extremely lethal virus. If you catch it, get ill, you really could die.” Remember the falling man, face down, in Wuhan? It's never happened anywhere else. It's pure theatre.
And it turns out that it's not a particularly lethal virus, if it exists at all. It's about the same as a bad seasonal influenza.
2. They used PCR testing repeatedly, off swabs up noses and throats, and led you to believe that these were highly accurate and able to distinguish a clinically infected person from someone that's not.
And even the inventor [of PCR], Kary Mullis, who's died, who won a Nobel prize for this technique, said you should never use it for this purpose. So I won't waste any more time [on this topic], but they're still using these damn tests, and they're not reliable; they don't tell you anything, really.
3. They also say you should wear masks, but masks have been extensively studied. Cloth masks, if anything, make you more likely to capture an unusual bacterial pneumonia, because you're breathing through a filthy cloth. And the blue medical masks are not masks, actually: they're splash guards.
Their purpose in hospitals is to stop blood and body fluids getting into the nose and mouth of the attending healthcare worker. They've never been for filtering your breath, and obviously they don't do so, but they told you to wear masks, and I think the purpose—certainly in me—it causes anxiety. I feel really awful wearing these things.
4. Then, they introduced lockdowns, where you were all to stay at home mostly, unless you were a poor manual worker, and then you had to go out to work—but the intelligentsia pretty much got paid to stay at home for very long periods of time: three months initially, in the case of Britain.
Lockdowns, they told us, would slow the spread of transmission of this virus, and lots of people thought it must obviously be so, because it is a disease spread from person to person. But it didn't chime with me, and I'm embarrassed to say it took me months to realise why lockdowns wouldn't work.
5.. And it comes to this next lie: the idea of asymptomatic transmission, that you could be bearing the virus in your airways yet have no symptoms, but nevertheless be able to spread enough of the stuff to infect a person nearby. That's not true. That's a flat lie.
Whenever a scientific advisor, medical advisor to a government, tells you things like like asymptomatic transmission, I want you to know that they're not mistaken; they're lying, because it's been studied and it's simply not true. I can supply a link which is an accumulation of statements by Fauci, a WHO doctor, and other people—actually, including me—that goes through this argument.
So if asymptomatic transformation doesn't occur—and I am certain it's epidemiologically irrelevant: I’m not saying it never occurs, but it's irrelevant—if it's irrelevant, why would you need to wear masks if you're well? Why would you need to test somebody who's not got symptoms? Why would you need to close your business or your school, or the economy?
So, again, they've lied to you, with the objective of both frightening you—and I think also, learning [this insight] from financially experienced people, the other objective was to begin to destroy the economy and the sovereign currencies, and I think that's a continuing objective.
6. They also lied to us and told us that there were no treatments for this respiratory viral infection. I will take my hat off to Dr Peter McCullough as a leader, but he's [merely] representative of very many brave physicians who pushed back on this nihilism. They have determined half a dozen really quite good therapies, used progressively: early on, you want to treat replication; in the middle phase, inflammation; in the terminal phase, coagulation.
And if you understand this multi-phase infection, you come to the conclusion—which is mine—that this is the most treatable respiratory illness ever. It's really quite surprising, but the the use of those treatments is denied almost all around the world, to the extent that people will be fined or even struck off as physicians. That’s another lie there.
7. Then they would say things like, “Well, we're not sure, when you've had it, whether you've become immune.” I would say Immunology 101 tells you that that's simply not true. We know that the default understanding would be: once you've shrugged off this virus, you will have taken high-resolution pictures of it, as it were, using your immune system, and if you see it again—or something related to it, like a variant—you will not get clinically ill; not for months, possibly many years. So that's another lie.
8. And the final lie—and we'll come back to this—is that the vaccines are safe and effective, but that's a whole whole other story.
I’ve said that the evidence of a supranational plan is the discarding of simple well-established pandemic preparedness plans and replacing them with this bunch of lies, and all the countries did it.
If someone would like to write to me with an innocent explanation for this, I’d love to hear it. I want to be wrong, but unfortunately I don't think I am.
Control
So if the motive is fear, I think the ultimate aim is control. We will come on onto this: the control mechanism, that we can see being installed all around us, of the so-called vaccine passports: a certificate first, on paper, and eventually a QR code on your phone, that tells anyone who needs to know that you have received the requisite number of doses of these materials.
We'll come back to this, but again, that's nonsense. Economic destruction, I think, is on its way. There was a person who's very experienced in the City of London, and I heard him phoning into a radio show three weeks ago, and he said, “I don't know anything about viruses.”
He said a lot about finance and talked about the amount of money—it's not even been borrowed, it’s just printed—this actually created new money with an IOU from the government: they have given certificates to investors. He said:
And that's because, as Catherine Austin Fitts tells us, this is a conspiracy led by the central banking clique and their clients to take over the world. I think once they've done that, destroyed the economy—again, I’m paraphrasing from Catherine—there will be a great financial reset which will have us using our vax passes — a digital ID — and central bank digital currencies, CBDCs, which you can look up. They are real and they are being talked about by all central banks. You won't like those; you really won’t. It'll be the end of cash and of any privacy of any transaction.
And I know I go further than many, but I’m really quite concerned that there's a serious intent to kill a very large proportion of the population of the world. Again, I hope I’m wrong, but all of the measures required to get to this point of control through vaccine passports — digital ID and also [the intent] to repeatedly vaccinate people: they certainly set the scene where a bad actor could introduce a gene sequence that will rob you of your health and kill you in a fairly predictable way at a fairly predictable rate per million doses. So if somebody does want to depopulate, the setup is so perfect that it isn't completely crazy [to notice this].
Before I move on to the vaccines—and this is a concern — I’ve had lots of people who have said to me:
And I suggest to them that they look for a video—on YouTube surprisingly—by a German journalist called Paul Schreyer. It’s a one-hour documentary called Pandemic simulation games — Preparation for a new era?.
And when you watch that, your last rickety defences that this isn't a well-organised, long-planned event will, I think, disappear, and your heart will be in your boots by twenty minutes in. Basically, all of the actors that you see around the table—including in, say, Event 201, that took place at the end of 2019—all of those players are currently taking the roles they had in the simulations, and all around the world, and are doing exactly the things that they did in the simulation. So those were the rehearsals, and there were more than a dozen of these damn things.
Anglocentric
And I think one of the bitterest moments for me was to realise that we were doing it to ourselves: that the US, UK, New Zealand, Australia and Canada—the Five Eyes—I think are the leading players. I’m not going to say Russia's not involved or whatever, but it looks like the Edward Bernays school of psychological management has been used by the military intelligence people: they've directed their weapons at their own people for two years, through all these lies, repetitive messaging, so that what we want to do is to wake people up—because if we don't wake up, we are finished as a set of liberal democracies.
I’m going to turn to the vaccines, but before I do that, I’ll say two things that are not original sayings but that strike me as very appropriate.
I’ve seen on many message boards: “When this all comes out, don’t ask me how I knew; ask yourself why you didn’t.” I mean, honestly, the the evidence that things are amiss, I think, is so stark that you literally have to avert your eyes not to realise that things are really bad everywhere.
And the other thing is an old saying—I’ve heard this before; it makes me chuckle a little bit:
And I’m afraid that’s what I’ve been: my job as a scientist was to spot faint patterns in sparse data—that’s what you do when you're trying to work out something that's new—and so I think I have been a couple of steps ahead, and probably sometimes wrong; but broadly, I think, it is, sadly, roughly what I’ve said.
Now, let’s get the slides up, because a colleague’s done an analysis that I think is quite striking when you see it.
Part II: Vaccine Damage
Published: January 12, 2022
This is the second instalment of a five-webpage transcript of Dr Mike Yeadon's testimony to the 86th session of Stiftung Corona Ausschuss, held on 7 January 2022.
In this transcript, covering the second twenty-minute block of his testimony, Dr Yeadon sets out the known folly of jabbing the entire population, and alleges a deliberate choice on the part of manufacturers to use a method of production that obviates measured dosing''.
So, to the vaccines. I worked for the biopharmaceutical industry for 32 years, so I think you can take it as read, but I'll say it again: I am in favour of innovative new medicines, provided they're well developed, used appropriately, and of course the profile is safe enough, considering the utility.
So if you were treating a terminal cancer that had evaded surgery, current chemotherapy, radiotherapy and so on, then you might be willing to take a drug that might kill five or ten per cent of the people, if it might stretch your life out for many years—especially if you're offered the chance of a cure. And with some of these gene-based vaccines, I think the original intent of people like Dr Robert Malone and others was indeed to treat things like that: you could put a protein from your cancer into one of these vaccines and force your immune system to recognise it and destroy it. And that could provide exquisitely safe novel chemotherapy.
But if you're going to treat effectively everyone on the planet—and you shouldn't do it anyway but that's certainly the state of intent—you need you need "safety, safety, safety," as Peter McCullough would say. That's your first concern, even more than "Does it work?": you need to make sure it's very safe, because you're going to be giving it potentially to billions of people.
I said earlier that my original training included toxicology. I was taught by at least two people that founded the discipline of mechanistic toxicity: Professor Jim Bridges and Dennis Park. They reminded us that in the 1950s, we didn't do toxicology in the drug industry. They would give it to two dogs and five chickens, and if the drug didn't kill them, they'd literally start giving them to people. That's how bad things were seventy years ago.
We had some strong wake-up calls at the end of the 1950s, early 1960s, with thalidomide, for example: it's a case that most people know about. At the time, they thought that babies were safe in the mother's womb, and so it really "wouldn't be a problem" if you gave a pregnant woman a drug. We now know that the foetus is is exquisitely sensitive to perturbations in their environment, and so we never, ever, give novel medical interventions to pregnant women. We’ll come back to that; we’re definitely doing that [with Covid injections].
Worrying design
So — because of my toxicological training and good understanding of what was required in new drug research and development—as soon as I looked at the [Covid] vaccines, I was really quite frightened, because they were a novel type. These have never been mass-dosed to human beings at all, so there would be no way of knowing what kind of unwanted effects might come about. And, of course, what you do is careful empirical study. You should do all of the possible studies. Your rule of thumb would be: if you can think of a worry, you need to show why why it's not going to happen, so you design an appropriate experiment. You have to try to "drown your own puppy," as we used to call it. It's not a good job, but you have to do it. You can't just hope "it'll be all right on the night"; it really isn't.
When I looked at the [Covid] vaccines, I had a number of concerns. One was: all four of them—AstraZeneca, Johnson & Johnson, Pfizer and Moderna—they all were fundamentally the same design, whether they used mRNA or or a viral-communicated DNA. They encoded only the spike protein: the bit sticking out from the ball-and-stick model of the virus that you've got. And I don't know to this day how they all chose just the spike protein, because we now know it's true that human immunity relies much more on understanding the depth of the molecular structure inside the ball than the spikes. So I thought it was bad, just the immunologically uneducated thing [to do], just to pick the outside part.
But secondly, [I developed concerns from] no more than half an hour of searching for research papers' abstracts and so on: not so much on coronavirus spike protein, because it's relatively new, but [research abstracts on] similar external proteins on other viruses. Within half an hour, I realised that all of them have some kind of biological properties that are unwelcome: they're not just for anchoring the virus to the surface of a cell, which they do do, but they're also biologically active — as you might expect, really They interact with the immune system and also with the coagulation system.
In fact, Wolfgang Wodarg led off, and I joined, a two-person appeal, a petition, to the European Medicines Agency to say, "Don't approve these vaccines at this time: here are a handful of concerns that we think are going to occur, and you need to slow down." And I think two of the four [concerns we enunciated] have been tested and proved correct, and the third one is looking pretty ropey.
So the design of them, I would say, was toxic by design. It was always going to harm people.
Not a vaccine
Next, [the design of Covid vaccines is] unlike a classical vaccine, which is usually a killed piece or preparation of the infective organism in a little bit of oil or alum, something like that. That's a unit dose, so you know how much you're injecting into each person. With these vaccines, we're giving unit dose of code. Now, that code could be copied into protein very efficiently, and might do so for a long time, in one person; in another person, it might be badly copied, inefficiently and only briefly.
So — I'm absolutely certain about this as a pharmacologist and toxicologist — by choosing this design, the range of outcomes is probably a thousand times worse than it would be for a conventional vaccine, because the actual amount of protein produced will vary by orders of magnitude more. And I thought that was the explanation for why it is that many people had no side effects whatsoever while others appeared to die.
People would say, "How could that possibly be true?" I just explained [to them] that with an encoded vaccine, an unlucky individual might take up large quantities of it in their hearts, in the coronary vessels, or in the cerebral veins in the head, and produce lots of spike protein for a long time, and most people [in that unlucky category] might get myocarditis or cerebral vein sinus thrombosis, and die; and in someone else, it might be spread around the body in a less dangerous place and not make so much spike protein.
I thought that was an adequate explanation, but I don't think that's the whole explanation any more. The reason I thought it was an explanation was, I made an assumption which I was entitled to make [in good faith], which is that the same stuff from a given manufacturer is in every single little glass vaccine vial. I believed — and was entitled to believe—that, to within a fraction of one per cent, we had the same consistent quality and purity in every single injection, and therefore the observed variation in in behaviour in people must be down to something such as what I just suggested.
But, as I'm going to come on to, unfortunately, we're now absolutely certain it's not the same stuff in every vial — and that means criminal acts are being committed.
What a vaccine is and does
Just before we come on to that: normally, a vaccine that you administer to a person would be one dose, sometimes two. There's never going to be a whole frame of them. [Yet] I'm seeing some countries already giving the fourth vaccine, and others have talked about an open-ended series! You need to know, vaccines are not like that. You do not need to be repeatedly dosed with something that would merit the title "vaccine". One or two doses, at most, [should suffice]. So it's more than that; it's not public health.
But here's the thing: a vaccine, or two at most, I think, will prevent you becoming ill with the pathogen against which you've been vaccinated. [The Covid jab model] doesn't do that, I'm afraid; it's not a vaccine. And [in a real vaccine,] as a consequence of protecting you against that organism—and it does that usually by killing off a new infection at an early stage, before you were even symptomatic—that would mean you should have low viral load in your airway, so that's what keeps you safe after vaccination or if you've acquired immunity.
The consequence of that is it usually reduces, if not stops, transmission. And we know now—[there's] lots of work in the literature—that people who've had this [Covid] virus are immune to becoming ill a second time from either the original virus or variants, and they don't transmit, either.
We know, we can see, what good immunity can look like. We've seen lots of cases of natural immunity. And authorities do agree: they concede that these [Covid] vaccines do not prevent you catching it; they don't prevent you growing the same amount in your airway as an unvaccinated person; and they don't prevent transmission.
So if someone's going to claim that [Covid vaccines] "reduce the severity of your symptoms", I'd like to know what black magic is invoked; because I've just told you, it goes to your airway, it grows in the same way, and transmits them the same way. I actually don't believe — there's no mechanism now for us to suddenly intervene and stop you getting ill — I don't believe it. So I think the most likely outcome now is, [Covid vaccines] don't do anything useful at all, but they are unfortunately really very harmful. They're certainly toxic.
VAERS
Just a brief introduction to one of the best tracking systems in the world: the Vaccine Adverse Event Reporting System, VAERS. It's a US system. It was put in place about thirty years ago, and anyone who has an adverse event following vaccination you—even if they not necessarily claiming it's necessarily caused by it, but in order to track the possibility—is urged to report that [to VAERS]. But unfortunately, the reporting rate is typically between 1% and 10% of adverse events.
Every piece of evidence has continued recently since the [Covid] vaccine started rolling out, and yet there have been more adverse events, and certainly many more deaths, associated just with the Covid vaccines than all the other vaccines in history that have been [registered] through this VAERS system.
So there is no question; it's public data, it's your database. It's not mine; I haven't put anything in it. 85% of the reports were put in there by a qualified healthcare professional. So it's not true, as some have asserted, that, "Well, people are just putting in spoiler claims, and they're not real." They are, actually; they're absolutely real.
Distinguishing correlation from causation
It's often said that correlation is not causation, and that's true: just because there's lots of reports doesn't necessarily mean that it's the vaccine. But there are things called Bradford Hill criteria [for causation]. You can look up the Bradford Hill criteria—I think there are eleven of them—and it gives you methods whereby you can determine whether the correlation is indeed causative or not.
I'll just give you a quick example: if there is acute toxicity in in the vaccine, then you would expect to see a spike in injuries and deaths in the first few days after administration; if there's no connection whatsoever, then you would expect a much more smooth, low-level profile that would not show much response to when you were vaccinated.
When you look at it, I think more than a third of the adverse events occur on the day of dosing or the next few days, and then it rapidly falls off. So that's one of the Bradford Hill criteria [for causation met].
Another one—and I'll only mention this one other—is plausibility. If you have a theoretical reason for believing that [a treatment] will make your left leg turn blue, and you go and look at the adverse events and find lots of blue left legs, that's much more compelling than if someone ended up with a sore elbow for which you had no predictive power. What I would say is, on these this occasion we believe that these agents cause so-called thromboembolic disorders.
So [one would predict] the effect of coagulation: you may bleed or clot, and so any vessels that are plugged up by clots—like strokes or heart attacks, deep vein thrombosis, or bleeding, like subarachnoid haemorrhage—any of those things are what you would predict. And, lo and behold, they are present in VAERS at enormous numbers, unprecedented numbers.
So the timing and the plausibility convinces me that these are causative; mostly, they are causative. And other people who are used to doing this—pathologists and others—have done a very thorough job, and unfortunately it's definitely causative. Large numbers, and it's causative.
Children
So when it comes to vaccines, wouldn't you expect—now, I put it to you—wouldn't you expect them to be deployed not just first, but only in the people who are at extraordinary risk from the from the pathogen? In this case, we know it's elderly people who are already frail. And [indeed,] that's how they started — but very swiftly, they started coming down to the working-age population: fifties, forties. And, as you're probably aware, we've now been trying to encourage people to get their children vaccinated.
Now, I don't know about your part of the world, but for Sweden and Germany I looked at the public record: not one healthy child has died as a consequence of being infected by this virus. Not one. So [how would you respond] if I tell you that there are novel technology agents that are being proposed to be injected into your child—a child who's not at any risk from the virus and who also is very poor at transmitting it to other people, because children generally don't get symptoms?
And I just told you earlier about asymptomatic transformation being a lie, so please, I'm begging you: whatever your neighbours say, or your schoolteacher or your government's advisor, I'm afraid they're lying or mistaken; you must not vaccinate your children.
So we should target these interventions to those who might benefit from them, because they generally will be willing to bear whatever the side effects are, in exchange for that benefit. So healthy younger people, certainly sixteen and down, really should not even have been on the map for vaccination, [firstly] because [if infected,] they survive; secondly, there are really good treatments, as I've mentioned, and so, with good therapies and people's strong immune system if they're younger and well, there was no need to vaccinate the world.
Pregnant women
And then, pregnant women. I have made a special examination of this from my toxicological background. I was just appalled when I heard a leading doctor—I think from the Royal College of Obstetrics and Gynaecology in London—[making this case]. The Royal College is meant to be the acme of medical quality, hopefully in ethics. And [yet] this woman appeared on national radio and proceeded to tell people that “if they were pregnant, they really should get vaccinated; and don't worry, these are perfectly safe.”
And I'll look you in the eye now and tell you that the studies have not been done to examine the safety of these vaccines in pregnancy. There's been no formal study, and there's no reproductive toxicology packages complete in the industry. I worked in the industry for 32 years; I can tell you we were not allowed to dose healthy female volunteers of child-bearing age without insisting that they used highly effective contraceptive methods, and generally we didn't do it at all. We just didn't do it until we had reproductive toxicology [results in], because we were all rightly fearful of the potential to damage a growing baby.
So it's literally nonsense: this is one of those things you should wake up to. Any listener knows that thalidomide changed the landscape forever in terms of precautions, in terms of medications in pregnant women, for reasons that we understand. And so, if your country's policy includes encouraging pregnant women to get vaccinated, when they are by definition relatively young and relatively well—they probably wouldn't have got pregnant [if not relatively young and well] and are therefore not likely to suffer severe effects of the virus—why would it make any sense to administer these experimental therapies?
Public health?
And then, worse than that: I've written affidavits and opinions to say there are two or three lines of evidence that would lead me to be extremely concerned for the potential for harms, and unfortunately, it actually does look like we were right about that. But I'm not going to push it any further.
My main point is just what I said in the last few minutes: it is just to say that if this was a public health measure, you would only administer these vaccines to people who could benefit most from it: the people who are most likely to get ill and die. And that would exclude healthy young people; it would certainly exclude children; it would definitely exclude pregnant women; and—here's the other thing—it would definitely exclude anyone who's had the virus and recovered.
There are scores of papers showing that people who've had the virus and recovered have a full complement of T cells of multiple types. That means that they will recognise the virus and any variants, and will remain well—and that is, in fact, the empirical observation.
So when you see your governments threatening the unvaccinated, including people who've recovered, [bear in mind that] they are more immune than than the people who've been vaccinated. So I just don't understand how anyone can go on about, "You're being anti-vaxx." No, no; I'm anti-conspiracy theory; I'm actually conspiracy facts. That's what's going on.
Part III: Hot Lots
Published: February 03, 2022
This is the middle instalment of a five-webpage transcript of Dr Mike Yeadon's testimony to the 86th session of Stiftung Corona Ausschuss, held on 7 January 2022.
In this transcript, covering 40' to 1hr10' in his https://odysee.com/@Corona-Investigative-Committee:5/Mike-Session-86-en:0 | testimony, Dr Yeadon gives his core presentation, with slides (reproduced below—not his own), on the massive variation in lethality between individual batches marketed by all three of the Covid "vaccine" manufacturers that are being administered in the United States.
A similar, much briefer, statement of the same material as the below was made recently by Dr Robert Malone, the inventor of mRNA vaccine technology. A more sceptical assessment of the quality of the same data is the ongoing work of Jessica Rose of The Truth Watercooler, particularly her 13 January and 20 January blogs.
So, then, moving on to the hot lots:
I mentioned earlier that I came up with an explanation for why many people have no side effects [from Covid injections] and [yet] some people get very ill and even die. That might be true, but the reason I even [took a while before I] thought of it was that you should expect pharmaceutical mass manufacturers to be good at least at one thing—and they are very good at this: consistent high-quality purity manufacture from batch to batch.
They’re very good at this because that’s what their business is: they manufacture tablets, capsules, sprays and injections in the billions of doses. If you think of something like Lipitor, a cholesterol-lowering drug: it’s given to a substantial minority of the population in older age—you know, one tablet a day, forever. They would have made tens of billions of doses. It’s not easy to make these [new Covid] genetic vaccines, but making a few hundred million, I think, would be absolutely in the wheelhouse of Janssen & Janssen and Pfizer. Moderna, at least, was a new company, so I can’t say; but I trusted that these companies were doing what I knew they were very good at doing: what they did for their business.
[But] then I stumbled across a couple of people independently who'd been doing their own analysis of the [US-specific] VAERS database. What they were doing, and no-one else seemed to have done it, was: they were pulling the vaccine batch or lot number—it might be eight digits, six digits, a mixture of alphanumeric characters—and comparing the profile of adverse events, comparing one lot to another lot with the same manufacturer.
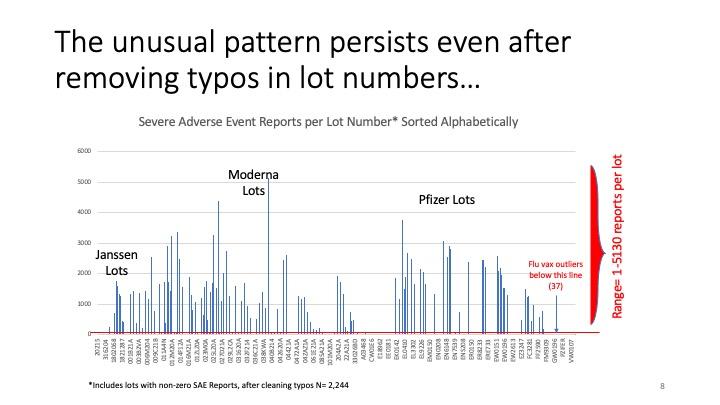
Their expectation was, it would be like a scattering of adverse events across all the [US] states and all of the lots—but they didn’t find that. This person [Craig Paardekooper] found that something like 90 per cent of the adverse events were associated with less than 10 per cent of the lots. [Note by UK Column: What is debated by some of those poring over the data subsequently is whether the batch numbers as supplied by the manufacturers are perhaps so riddled with typographical errors, such as mistaking zeros for letter O and ones for letter I, that batches might be inadvertently lumped together in this analysis. Yeadon does address this point below.]
I remember seeing that some months ago, and I immediately knew the significance of it, because—as I’ve said—although I’m not in any way a manufacturing expert, I worked for decades with people who were, and I knew their pride and the necessity of meeting their anti-adulteration regulations, which require tremendously reproducible product from lot to lot.
I’ll just briefly describe the manufacturing of medical products. It proceeds in two steps. The first step is to make the active molecule: in this case it would be mRNA or DNA with a “bite”, with an attenuated virus. We would think of that as the first step. It’s the drug substance; it’s the actual active component. And then, once you’ve got that, it will generally be formulated in some way. In this case, it’s going to be in some sort of dilution material; it might be medical saline sometimes, though it’ll be mixed up with binding agents, colourings, lubricants, shiny coats on a capsule or tablet. That’s called “drug products”. So the first step is to make the active component and the second step is to formulate it and finish it with the drug product.
Now, each of those steps is associated with a series of acts. You might start with a raw material, two raw materials, and then warm them up to manufacture a third product, and then purify that. And that might be a step. The manufacturer submits to the regulator its pharmaceutical production plan, and each of those steps has to be gone through by experts and the regulator. They agree that the steps are appropriate and that the limits—the range of outcomes on testing—are appropriate. And only if they are [found appropriate] would you be permitted to go to step two, three, four, five, until you’ve completed all the steps.
I’m elaborating a little bit to tell you that they don’t just throw everything into a bucket, like home brewing beer: stir it a bit, put it in the bucket. All this is done with just incredible levels of control—as you'd expect: you want it to be reproducible. So the effects of following what’s called good manufacturing practice, or GMP—as required by a medical regulator even for an emergency-approved product—[are that] it should be the case that the lots effectively contain the same stuff wherever it was made and whenever it was made: it’d be the same stuff. And I know they’re capable of doing that.
Now, if that’s true, [then] if you draw a lot at random from the VAERS system and examine the outcomes, the performance—that is, the number of people who’ve reported adverse events—it ought to be pretty similar from batch to batch to batch.
If it’s very different, I’m afraid I can tell you with certainty—I would be able to prove this mathematically if needed, in court—it’s not possible to go from two or three adverse events reported for a given lot and another lot [to] have 5,000 adverse events. It’s not possible if you only vary the products a little bit.
You might imagine, “Well, they’re doing this at speed and it’s novel; Mike’s being a bit hard on them.” No. if you only have a small difference, you only get a small difference in the performance. If you go from effectively nothing to the worst outcomes ever reported to VAERS, I am prepared to state and to prove that that means it’s not the same material in the lots that produce bad side effects.
You may not appreciate the significance of what I just told you, that it’s not the same stuff. If you thought [what everyone’s been getting] was the Pfizer/BioNTech Covid-19 vaccine that was used in the clinical trials: some of the batches contain something different. I cannot know what it is, but it’s definitely not the same stuff. As the above slide sets out, if it contains the same product, the performance should be pretty similar; just a little variation.
I'm not the analyst; in fact, it's an irony I'm the person speaking. I'm the only person [in Team Enigma] not capable of doing the information technology. But one reason I'm speaking is because of my deep experience of pharmaceutical research and development, and knowledge from people who are experienced about manufacture. What I've described is true.
Also, the people doing this work are self-starters: we've got a degree of independence and we're all speaking out because something awful is happening.
As I mentioned in my introduction, it's quite normal, I'm afraid, for every medicine to have some kind of side effect. I think it was a very old physician, Paracelsus [of the Renaissance era], that said, "All medicines are poisonous; it's just a question of dose." That's kind of true: rat poison used at very low doses, or its modern analogy, can be really useful to thin your blood.
But that means you need consistency from dose to dose to dose. And it was true that in the first half of the twentieth century, many pharmaceutical outfits—that were probably quite small at the time—were occasionally careless, if not outright reckless, and adulterated products. That is, products were not the same from tablet to tablet or injection into injection. And so that brought about these FDA regulations that relate to what's known as adulteration. Really, it's about reproducibility, purity and so on.
For the lawyers, this is very important. My colleague who put this together taught me something I didn't know: those [early twentieth-century FDA] regulations were formed to make sure that badly manufactured products were never again foisted on the public. They said that "if it's not made as you have described, and made consistently—so more than a tiny variation fraction of one per cent; perhaps that's allowed, batch to batch—we will declare it to be adulterated."
And the thing is that adulteration per se—manufacturing and release of materials which I assert, and others in this team agree, are performing very differently one from another—by definition means that it's not the same stuff. By definition, it's adulterated, and I think by definition that they have broken various laws.
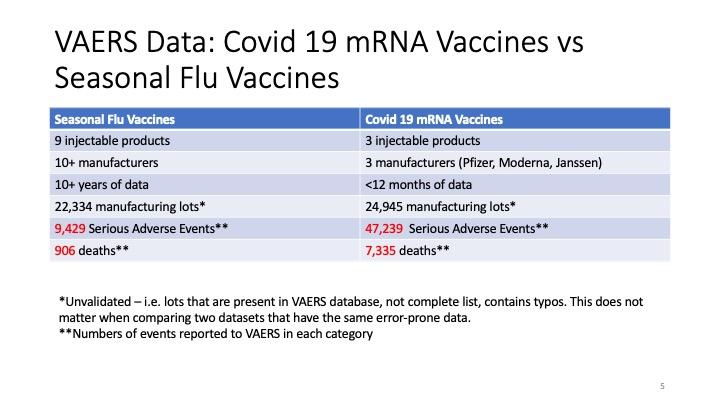
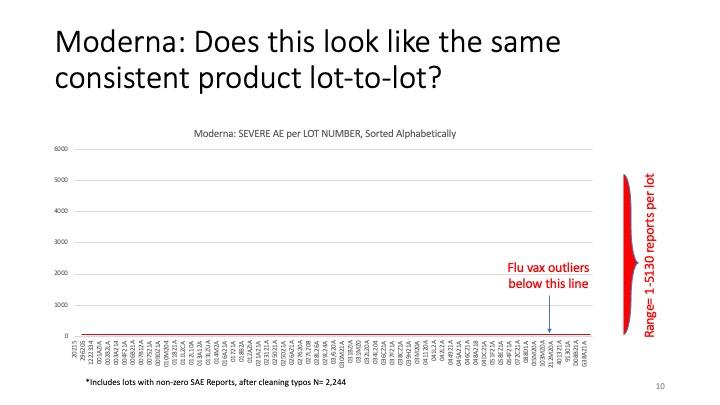
This slide is really important. Again, the initial analyst just looked at the Covid-19 lot numbers and found that the side effects were not uniformly, not even pseudo-uniformly, spread across the lots. But what this other colleague has done is to say, "Well, let's look at the thing that's most comparable." So she looked at all the injected products against influenza.
As you can see, it's decades of data and it's about 22,000 to 23,000 manufacturing lots, and if you look to the right, the "mRNA vaccines" column, five lines down, a similar number: 25,000, so they're similar numbers of lots [being compared between flu jab and Covid jab adverse reactions].
But if you look at the serious adverse events, you can see something like a five-fold difference there! From 9,429 to 47,239. And in terms of deaths, I think it's like eight times worse. So something very peculiar is happening.
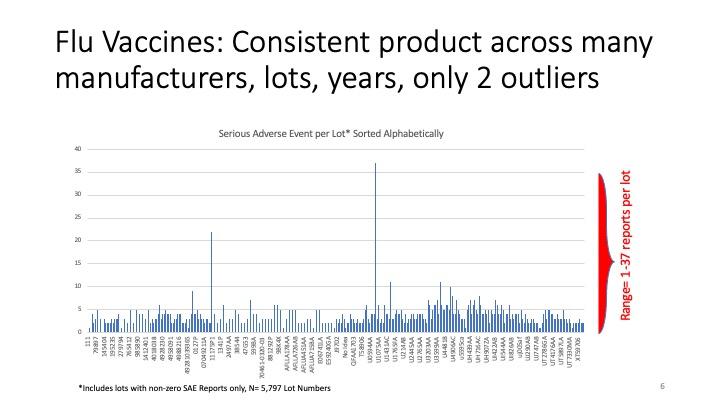
Now, these next couple of slides are the crucial ones. Along the bottom, there are the—meaningless to me — [batch] numbers associated with all these injectable flu vaccine products over many many years, and on the vertical axis are the number of serious adverse events. You can see there were just a couple of outliers: one with about 22 serious adverse events.
A serious adverse event is something that would bring you to hospital, extend your hospital stay, could threaten your life, require urgent intervention to save your life, something like that. These are not a sore arm or a bad headache; this is something really bad. But [there are mere single-digit numbers of adverse event per flu jab batch], with the exception of the one on the left there, with 23 serious adverse events. A lot might contain several tens of thousands of doses.
We don't know what it is every time, but what we can say is that since—as I’ll show in a moment—the number of adverse events [with Covid jabs] can vary thousandfold, it's not possible for the difference in batch size or lot size to be the whole explanation for the differences. It might contribute to it, but we've done some preliminary examination where we have managed to find out exactly how many doses there were in a group of lots; and when we looked at the relationship between the number of doses in the batch and the number of adverse events in the batch, there's no relationship. So that’s not the driver.
With the flu vaccines, there are just two lots where something went wrong—we don't know why—and there were a relatively large number [of serious adverse events]: 22 and 37. But look at the rest: there are hundreds and hundreds; thousands; tens of thousands of lots [of flu vaccine lots in VAERS] where, on average, my eye is telling me that the smooth average is around four serious adverse events per lot. But more importantly than that, I think, you'll agree it kind of looks like static: just background noise.
Remember, if you dose a large population—you could dose them with saline too and get this effect, because people do get ill [of various causes anyway]—you might put on red socks today and have a heart attack; obviously, the red socks didn't cause your heart attack—but if you were tracking the relationship between your new product with socks and side effects, you would end up with a product with a profile that looks like this.
So side effects associated with a an intervention does not necessarily mean that it's bad. As I mentioned earlier, this sort of correlation is not causation. But—and this is really good work by my colleague—I wanted to show you what we think a normal, well-manufactured, consistent, high-quality product looks like in the real world, when you give it to millions of people over time.
So now, with that established, the baseline is around four, and the highest value [of adverse reactions with flu jab lots] was 37.
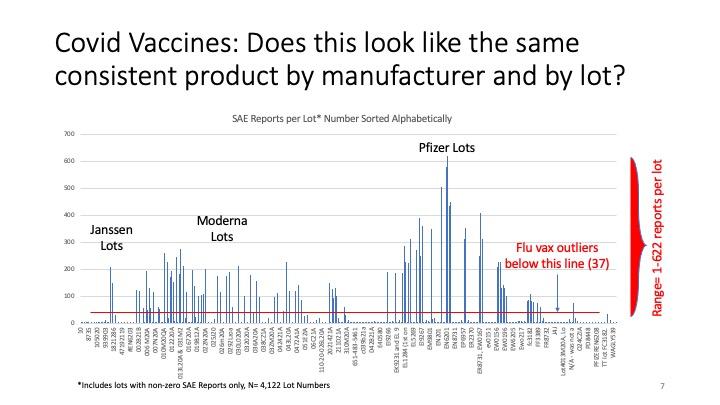
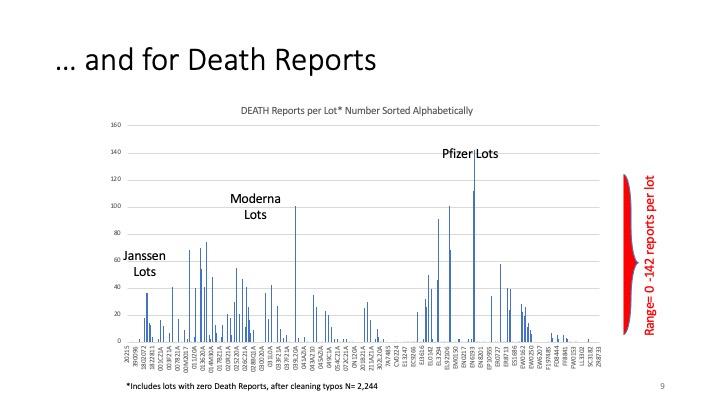
So this, by now, should start to take your breath away. These are the Covid vaccines. There are three manufacturers, because it's the US commercial utilities. It’s just these three. We don't know about AstraZeneca.
Remember I said that the rolling average was about four adverse events per batch? Well, you know, the scale on the Y-axis here is thicker, the thin blue line [for the Y-axis] at the bottom is more than four [the scale is such that four adverse events would not show up on it]! And the red line—this is the worst ever you can see—there was a single case out of 22,300 flu vaccine batches, and that was 37. But really, that's probably way over what the representative was. The representative [number of adverse reactions per batch of flu jab] was somewhere around four.
But that's the top [ever for flu jab adverse reactions]. Look how many batches of Covid products are worse than that! And yet, let me just point out, for example, right in the centre there: that batch number looks like it [has only] either one or two [adverse reactions]. [UK Column note: The batch number which Yeadon reads out from the bottom axis of the slide at this point is not consistent with the format of any others, happens to be in North American telephone number format, and turns out to be the telephone number of a medical clinic in Minnesota, so it is possible that it is not actually a manufacturer's lot number.]
And then its neighbour [has] one or two; its neighbour, one or two; its neighbour, one or two. But then, suddenly, you come on this one here: EN6201. It looks like it's six hundred serious adverse events. Again, if you had a serious adverse event yourself, you would think, "Thank God I didn't die." It's quite close to death. And look at the number of them.
There's a number of things I want to point out here. One is the extreme level of side effects that we're seeing: orders of magnitude [worse than flu jab adverse reactions], I would say. Just the rolling average here is looking like, I don't know, between 100 and 200, instead of four!
[We see] that these are really toxic products. They really are toxic products. That's bad enough, but—as I argued—if you're a cancer sufferer, you might accept a dangerous intervention if, on balance, it could extend your life or its quality by a year or so.
But these products have been given to the general public, most of whom are perfectly well. That's the normal deal with the vaccine: you're perfectly well when you turn up at the doctor's office, you get an injection, and you leave and you're still perfectly well, and all that's happened is you've acquired a defence against a specific pathogen. That's the deal.
What we shouldn’t have is that you occasionally get seriously ill and some of you die. That's not a good deal. [Yet] that is what is happening from these products, and they're being pushed on everyone, when—as I've argued—if you're recovered, infected, you're immune; if you're a child, you're not vulnerable to the virus; healthy young people [do not need it] and for pregnant women we do not know that it's safe, and we should not, on the precautionary principle, be administering it [to them].
And yet your governments are pushing these on you. it's not a public health measure. If it was a public health measure, the three or four things I’ve just said would be true. It's not a public health measure.
And [bearing in mind] all I said earlier about discarding normal pandemic handling plans and replacing them by absurd lies, that have had the effect of frightening people (and we think that that was the objective): now you've seen this information, and your economies are on the verge of absolute extinction.
And so I think that's the evil triumvirate: frighten the people, damage the economy, force them—persuade them or force them as necessary—to accept these injections, some of which are killing people.
Why would they want to do that? And this is why I got to the conclusion I [reached]. I racked my brain: there may be other explanations. It's not money, by the way. The pharmaceutical companies, of course, are having an absolute field day, a high water mark in terms of profitability. That cannot be the motive; it’s the effect of using Big Pharma to drive these products into the population. It can't be the motive.
Why can't it be the motive? Because there are huge numbers of industrial sectors that are absolutely [driven] almost into the ground: the airline industry—I don't know how they're surviving, almost two years of non-normal operation; hotel and catering, holiday trade; and all of these things. So remember that the only people who could possibly make this happen, or at least have to agree in order that this happens in their world, would be the owners of the people, what Catherine Austin Fitts called "Mr Global": global big capital.
So I'm absolutely sure that money alone, profit alone, is not the motivation, because [while] there might be a couple of sectors doing really well [out of Covid], eight sectors are doing so badly as to more than outweigh the benefits that accrue to the drug companies.
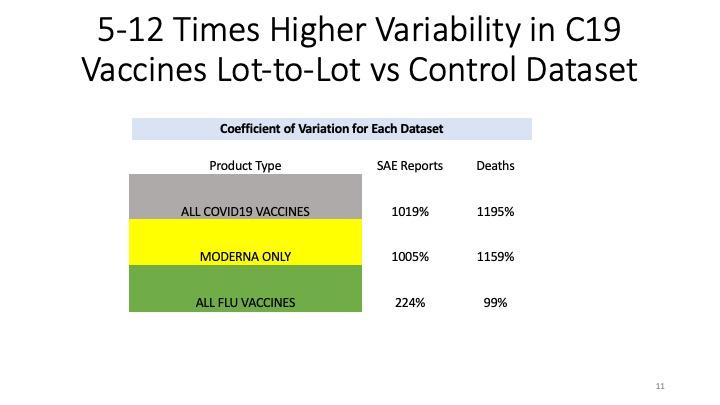
But let's just go back to the slide, because it's not just this extreme toxicity; it's the variability.
Now, let's just look at the Pfizer bumps, because there's a nice range there. "Nice" is the wrong word, sorry; I'm sounding like a scientist. These are people. These are people who've suffered, and some of whom have died. But as you cast your eye across the axis at the bottom, you can see that some of the [batch] numbers there are associated with very small numbers [of adverse effects]. They're so small, you can't see it registering on the thickness of the Y-axis marking zero. And yet, close to them, there are a whole bunch of batches that have got 400 to 600 serious adverse events per lot, and they're roughly the same size.
That means it's not the same product that's got this Pfizer Covid-19 vaccine that it says on the box or or on the vial. It's not the same stuff. It's not the same stuff. I'm certain it's not; an assessment. It's not "maybe"; I'm absolutely certain.
There is something called the law of mass action, which applies to all biological properties I've ever seen. And if it does come to court, I will walk you through the history of that: why it is that shape and why this means it cannot be the case that these middle Pfizer lots are the same material as the ones immediately to the left and to the right.
These drug companies are highly professional outfits. They know how to manufacture reproducibly, and we saw that with the flu vaccines over decades. They know how to do it; they haven't done it.
I'm afraid I've come to the conclusion that they're doing it on purpose, because they're so professional, and after a year they know this data. This data is their window onto the world. They can go into VAERS; they can filter for their own products, and their own lot and batch numbers; and they can see what's happening. They know. So the fact they haven't stopped this tells me that they're at least okay with it—and I fear that this is deliberate.
Why might it be deliberate? Well, as as we have seen over the last two years, Big Tech firms like Google, Facebook, YouTube, Twitter and so on have persistently said, "We're not having anyone making a comment or a recording that disagrees with what the public health officials say, and we're going to call that 'misinformation', and basically we're going to censor you, and maybe de-platform you."
What that means is that a qualified person like me—and I promise I have no axe to grind whatsoever, other than telling you what I think is true, which is that we're facing a global crime—people like me cannot speak to the public, because the tech companies have decided not to let me. That's true of mainstream TV, mainstream radio; I've only ever appeared on [mainstream] radio when they where they maligned me. They've told lots of lies about me, so I then threatened them, and then they deleted the recording—which tells you something: wasn't it that I was correct?
So it's the combination of Big Tech and Big Media—and by that, I mean mainly TV around the world; they control what's coming into your house, so if you just turn your TV on over the last two years in the same way that you ever have done, you're only going to hear a one-sided [presentation]. And in my view, it's mendacious; it's a completely misleading description of what's going on. You'll never hear things like this. And you should. You should. You should see both sides of it.
The fact you're not allowed to, I think, tells you that they know there's something bad going on, and they're going to make damned sure that people like Dr Mike Yeadon and Dr Robert Malone and Dr Peter McCullough and so on will never darken the studios of the BBC or CNBC—because if we were given an hour, I think we could destroy this story. Easily. I think we're plausible: we're being honest, and gain absolutely nothing from making up the stories I'm describing in horror.
I've said that the variability is extreme, and I've said that the media controls the message, and they censor people like me. If they want to tell you that "there's a nasty variant that's just come along that's killing more people than previously", you've no way of knowing if that's true or not. And I don't think you should trust anything they say about this, because they've definitely lied about everything else I've been able to hear.
But if they said "there's a new variant or a new virus that's ten times more lethal than Covid, and don't worry, the innovative pharmaceutical industry has rustled up a new vaccine; run and get your top-up, your booster, your new vaccine"—what happens if they choose to give you the one that's called EN6201 instead of EN1201?
Well, the answer is, probably thousands of people are going to die. And imagine all the manufacturers doing that. And across the world, all the time, the media is giving you a very frightening message—and the appropriate response, if these guys were being honest, would be, "OK, let's deploy these vaccines as we tune them and so on." But it's all lies; it's all misleading; and I worry [about] what you've seen in front of you there.
I've described it to other people by saying, "I'm worried that this is the calibration of a killing weapon." [What if, soon,] there are vaccines that would be, say, ten times more lethal than Covid [jabs]—so killing one in a hundred people instead of one in a thousand, roughly: they could just move along and just deploy [bad] batch X or batch Y or batch Z, and that [mass death] is what would happen.
And I've got no reason to make this stuff up. I've never been a conspiracy theorist; if anything, I'd be the sort of person who would chuckle at other people having conspiracy theories, and of course, now I realise what a mug I've been for the last 61 years for believing what I've been told.
So the bottom line—you can see it from here: it's not the same stuff in each glass bottle. That's an offence, in all sorts of ways, against adulterated drugs law (21 U.S. Code §351). It cannot be accidental, because they are professionals that know how to manufacture consistently.
It's not possible [to admit the excuse] that "This is small variation in product because it's an emergency situation and difficult to make." No, the law of mass action would mean that in order to get these enormous differences in “performance”—you know, serious adverse events—you would have to have a very a sizeable difference—I would say a ten- to hundredfold difference in an active ingredient—if there was if there was an active ingredient that produced these side effects.
I'm confident, and we did the experiments; I'd be roughly right [with this prediction on that basis]. I've done hundreds of experiments like that—not with people, of course—and [determined that] we'd need to go up in dose by a good 300 times to go from baseline to these numbers. I'm absolutely sure about that. I’d bet a lot of money on it.
So, because they're good at manufacturing, and because this data has been available to them all the time—they can look as the VAERS data comes in, so they've known about this, and that means they accept it—it's [therefore] either intentional, or if whatever is [in the shots] has proven too difficult to manufacture, they should still not be allowed to discharge these, as it were, into the public environment, because they're very lethal.
Some people have said to me, "Mike, these are brand new products, as you've said, and early on we heard that the Pfizer product had to be stored at, like, -80ºC, so that means they're rather unstable. Maybe, Mike, what's happening is, they're just going off occasionally. You know, bad handling; people not used to what's called a cold chain; things like this."
Well, I don't think that's true. For one thing, when products degrade, they generally lose activity: a piece of it falls off. If you imagine a car degrading, you might lose one wheel and the top part of the engine. It doesn't suddenly turn into a lethal flying machine; it will lose function, and that's what I would expect to happen.
Now on a one-off, yes, maybe a novel product like this might break in half and you end up with two supertoxic bits of mRNA; but we're seeing the same thing with three products made by three different companies, and we're seeing two different technologies: Moderna and Pfizer are mRNA; the Janssen is a DNA [technology]. No, it's not possible.
I’ve just said the rule of thumb is that degradation results in a loss of functions, not acquisition of extreme exquisite toxicity. And we've got three products and two technologies doing that? No, that's not the explanation. Whoever's doing this—and here's the thing: I have no idea what it is they have done—but I'm more frightened of these vaccines than I was before seeing this work with my colleague.
I think that's the long and short of it, really. All of the early stuff, you're being lied to, and I can prove that on several occasions. I would like to direct people who haven't seen me before to my interview with Del Bigtree on The Highwire, and that, I think, will educate you on what I was seeing as the principal lies.
And I certainly would like to attach a sixteen-minute link with three or four people talking that will provide you convincing evidence that the authorities knew that asymptomatic transmission was complete garbage. And if that's true—and it is true; it's garbage—everything else falls to pieces.
And when we come to the vaccines, if they were a public health measure, they'd be directed only to the people who could get most benefit from it, and never to children, healthy young people, pregnant women, and those who have already recovered. And yet a coach and horses has been driven right over those.
So that's about where we are. The reason I'm here is, I want to work with anyone—through Stiftung Corona Ausschuss and anywhere else—that can help wake people up, because I don't know how to fix this, but if enough people say, "We've had enough now; we're not going to comply with it any more," [it will end].
I noticed in northern England, there were a group of several thousand children from secondary school in Lancashire who formed a union, and they just said, "You know what? We're not wearing the masks any more, and no, we're not going to put these cotton buds up our nose twice a week. Not doing it any more." And that's all we need to do, because I am telling you there is no unusual threat in your environment except from your government and their policies and the pharmaceutical industry. There's nothing going on other than the sort of psychological warfare, and the economic damage, and then these wretched vaccines
So we can we can still take our old normal back—hopefully in a better form—but it requires us to just take a little courage in our hand and say, "I do not comply any more. I do not comply." And you're not doing anyone any good by complying; you're not saving yourself; you're certainly not saving your children.
That's all you need to do, and they can't arrest everybody, right? One or two people decide to demonstrate, they could be arrested; if ten thousand schoolchildren say, "We're not going to school with masks and testing," and they just cross their arms and say, "What are you going to do, then?", that's how you take it back. That's how we take it back.
Tags: TheBigCovidLie, EightCovidLies, BigPharma, Vaccines
This page may have a talk page?.
Access and use of this site by any means implies consent to the Agreement of Use. © Hellene Sun